RESEARCH ARTICLE |
https://doi.org/10.5005/jp-journals-10033-1502 |
A Prospective Observational Study on Single-incision or Conventional Three-port Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair
1Department of General Surgery and Allied Superspecialities, Government Medical College, Srinagar, Jammu and Kashmir, India
2–4Department of Surgery, Government Medical College, Srinagar, Jammu and Kashmir, India
Corresponding Author: Safoora Wani, Department of Surgery, Government Medical College, Srinagar, Jammu and Kashmir, India, Phone: +91 9697901442, e-mail: safoorawani@gmail.com
How to cite this article: Wani YH, Attri MR, Gilkar I, et al. A Prospective Observational Study on Single-incision or Conventional Three-port Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair. World J Lap Surg 2022;15(1):77–86.
Source of support: Nil
Conflict of interest: None
ABSTRACT
Aim: The study was aimed to describe the outcome of single-incision laparoscopic surgery (SILS) and conventional totally extraperitoneal (CTEP) repair for inguinal hernias in terms of the following: (i) operative time; (ii) rate of conversion to open; (iii) postoperative complications; (iv) hospital stay; (v) cost; (vi) time until return to normal daily work; (vii) postoperative pain score; and (viii) cosmesis.
Materials and methods: The present study was a prospective observational study done at the Government Medical College Srinagar, Department of surgery and allied super specialities.
Results: The mean operating time in the CTEP group was 41.2 and 42.8 minutes for SILS TEP. Overall complications were slightly more in CTEP. The mean postoperative hospital stay was 19.2 and 21.8 hours in CTEP and SILS TEP, respectively. The average time to resume normal work was 3.7 ± 0.8 days in CTEP repair and 3.3 ± 1.2 days in SILS TEP repair. The mean visual analogue scale score at 6 hours in the CTEP group was 3.1 ± 2.8 and in the SILS TEP group 2.8 ± 0.8. The mean cosmetic result was 4.1 ± 0.9 in the SILS TEP group.
Conclusion: Laparoscopic repair of inguinal hernias is associated with good results in both techniques. SILS TEP inguinal hernia repair using conventional laparoscopic instruments is a safe and feasible alternative to CTEP in experienced hands. The outcomes of SILS TEP for operation time, postoperative complication, hospital stay, time until return to normal activity, and rate of conversion to open are comparable to CTEP. However, the approach provided an advantage in terms of cosmesis and postoperative pain.
Clinical significance: SILS TEP although having a learning curve and difficult to use in large/complete groin hernias is a good technique for use in small hernias using routine laparoscopic instruments in a resource-limited setting with significant outcome in terms of cosmesis.
Keywords: Hernia, Intraperitoneal onlay mesh, Laparoscopic, Laparoscopic hernia repair, Mesh, Mesh repair, Single-incision laparoscopic surgery, Single-port, Single-port access surgery, Totally extraperitoneal, Transabdominal retromuscular, Ventral.
INTRODUCTION
The word “hernia” is derived from the Latin term meaning “rupture.”1 Hernia is defined as an abnormal protrusion of an organ or tissue through a defect in its surrounding walls. Hernia can occur at various sites of the body, most commonly involving the abdominal wall, particularly the inguinal region. The most common sites are the inguinal, femoral, and umbilical areas, linea alba, lower portion of the semilunar line, and previous incisions sites. Strangulation is the most common as well as serious complication of hernia and is seen in only 1–3% of groin hernias.2
Inguinal hernias account for 75% of abdominal wall hernias, with a lifetime risk of 27% in men and 3% in women.3 Inguinal hernias are classified as direct or indirect based upon the site of herniation relative to surrounding structures. The definitive treatment of inguinal hernias is surgical repair.
The goals of herniorrhaphy include the following:
Minimizing operative and postoperative discomfort for the patient.
Achieving an effective repair,
Ensuring the lowest possible recurrence rate,
Permitting a rapid return to normal activities, and
Performing a cost-effective procedure.
Over the past century, multiple methods of repair have been used. The techniques have progressed from open repair to laparoscopic approaches.
Over the last few years, with increasing demand of better cosmetic results along with better surgical outcome, a newer technique has gained interest among the surgeons. In 2009, the first case of single-incision totally extraperitoneal inguinal hernia repair was reported.4 However, evaluating this newer technique with respect to the three-port conventional totally extraperitoneal (CTEP) repair in the management of groin hernias has not been thoroughly published to date.5–7
MATERIALS AND METHODS
The study was a prospective observational study of patients with groin hernia (Fig. 1). There were two study groups. One group of patients has undergone single-incision totally extraperitoneal inguinal hernia repair technique and the other via three-port CTEP repair procedure. The two groups were then compared based on intraoperative and postoperative parameters. The main aim of the study was to observe these two techniques in terms of the following:

Fig. 1: Inguinal hernia (preoperative)
Operative time
Rate of conversion to open technique
Postoperative complications
Hospital stay
Cost
Time until return to normal daily work
Postoperative pain score
Cosmesis
The study was a prospective observational study. The study cohort was admitted for elective groin hernia surgery in surgical wards of SMHS Hospital Srinagar over 2 years. Patients above 18 years of age, irrespective of the gender presenting with groin hernia were evaluated as per a predetermined proforma.
Following patients were excluded from the study.
Age below 18 years.
Complicated hernia.
Previous lower abdominal or pelvic surgery.
Contraindications to general anesthesia or laparoscopic surgery.
Associated medical comorbidities, like COPD, uncorrected bladder outlet obstruction, and uncorrected chronic constipation.
The patients were admitted after being evaluated on outpatient department basis. Baseline investigations followed by preanesthetic checkup were done in all cases. Preoperative instructions were given and made understandable to the patient in his/her language. Written informed consent was taken before each procedure. Prophylactic antibiotic (injection ceftriaxone) and tetanus toxoid dose were administered before the procedure in each patient. Surgery was performed on a routine elective basis after proper investigation as per following operative techniques.
Single-incision Totally Extraperitoneal Inguinal Hernia Repair Technique
Under general anesthesia, the patient is placed supine with both arms adducted. Later the patient is placed in the Trendelenburg position with the side contralateral to the hernia site tilted down. A 25-mm subumbilical incision is made, followed by dissection of the subcutaneous tissue down to the rectus abdominis sheath. An incision approximately 3 cm in length is made over the anterior rectus sheath and opened, blunt dissection using a finger or gauze is performed between the rectus muscle and the posterior rectus sheath to create a preperitoneal space. The single-port self-retaining access device through which three trocars are inserted is used to maintain the inflation of the preperitoneal space with carbon dioxide gas (Fig. 2). Carbon dioxide is insufflated to a level of 15 mm Hg.
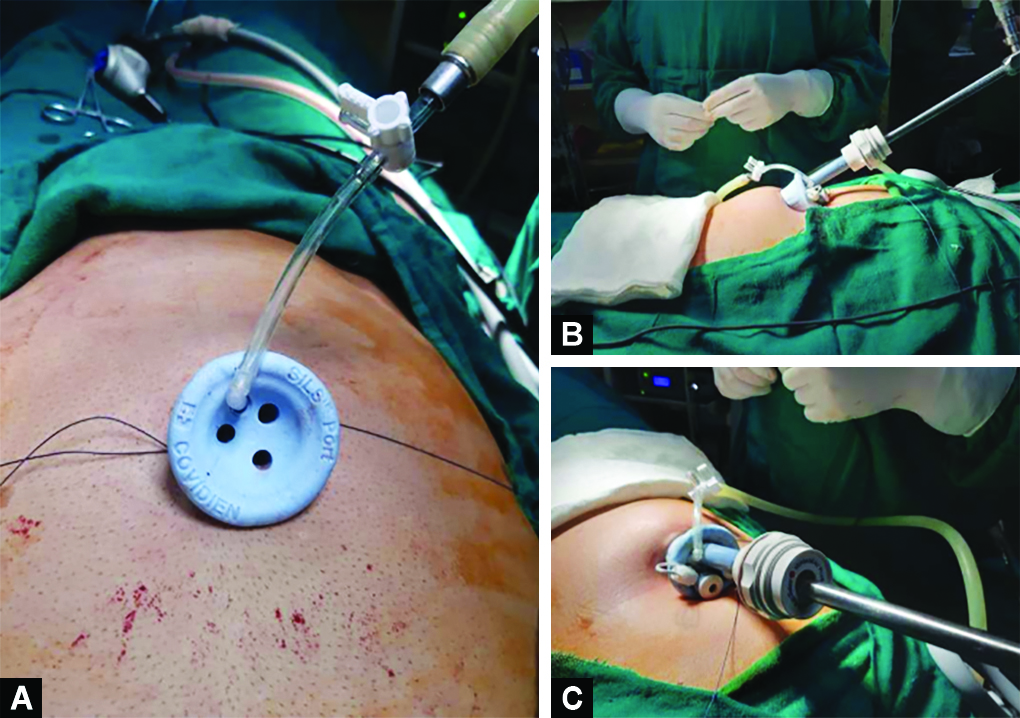
Figs 2A to C: SILS port in use
The preperitoneal space is gradually dissected using conventional laparoscopic instruments (initially a 0° telescope) without a dissection balloon (Fig. 3). The boundaries of dissection are similar as for CTEP procedure. A polypropylene mesh is introduced through the 12-mm port half rolled (Fig. 4). The mesh is unrolled along the floorcovering the inguinal floor and fixed (Figs 5 and 6). The fixation is performed by the use of three absorbable tacks—at the pubic bone, at Cooper’s ligament, and above the iliopubic tract. After completion, the preperitoneal space is deflated with care to avoid displacing the mesh. The anterior sheath is closed with a 2-0 Vicryl suture, and the skin with a 3-0 silk suture.

Fig. 3: Intraoperative picture while dissection of sac

Figs 4A and B: Mesh used for the procedure

Figs 5A and B: Placement, unrolling, and fixation of mesh using absorbable secure straps

Fig. 6: Complete unrolling of the mesh over the myopectineal orifice of Fruchaud
Postoperative Care
After the operation, patients were shifted to the respective wards and monitored. Injectable diclofenac sodium 75 mg was used for immediate postoperative pain relief. In both techniques, patients were made ambulatory and orals started on the same day of operation. The patients were discharged from the hospital as soon as the patient became ambulatory and tolerated orals and were pain-free. Patients were followed up at 1 week, 2 weeks, 4 weeks, 3 months, and 6 months.
The following parameters were recorded during our study:
Information on gender, age, comorbidities, and past surgical history.
Hernia characteristics, like type of hernia whether indirect, direct, femoral, side of hernia, unilateral or bilateral, primary, or recurrent, were noted.
Duration of surgery.
Rate of conversion to open technique.
Pain score at 6 and 24 hours after the procedure.
(0—no pain, 2—least pain, 4—mild pain, 6—moderate pain, 8—severe pain, and 10—worst pain possible)
Postoperative complications, like seroma, hematoma, and urinary retention, if any were recorded.
Time until return to normal (nonstrenuous) work was noted.
Cosmetic results were graded subjectively 1 month postoperatively using the following range of choices: 5, very satisfied; 4, satisfied; 3, acceptable; 2, dissatisfied; and 1, very dissatisfied.
Statistical Analysis
Data were expressed as average and percentage. All the inferences for comparison within the group were made using Fisher exact test, Chi-square test, and unpaired Students t-test. A p-value of <0.05 was considered significant.
RESULTS
Age Distribution
CTEP Group
In our study of 30 patients, CTEP group consisted of 15 patients. There were two cases between the age-group of 30–40 years; four cases in the age-group of 41–50; eight cases between the age-group of 51–60; and one case above the age of 60 years. Majority of cases belong to age-group of 51–60 years with mean age of 50.67 as is shown in the Table 1A and Figure 7A.
| Age-group | Number of patients |
|---|---|
| 30–40 | 2 |
| 41–50 | 4 |
| 51–60 | 8 |
| >60 | 1 |
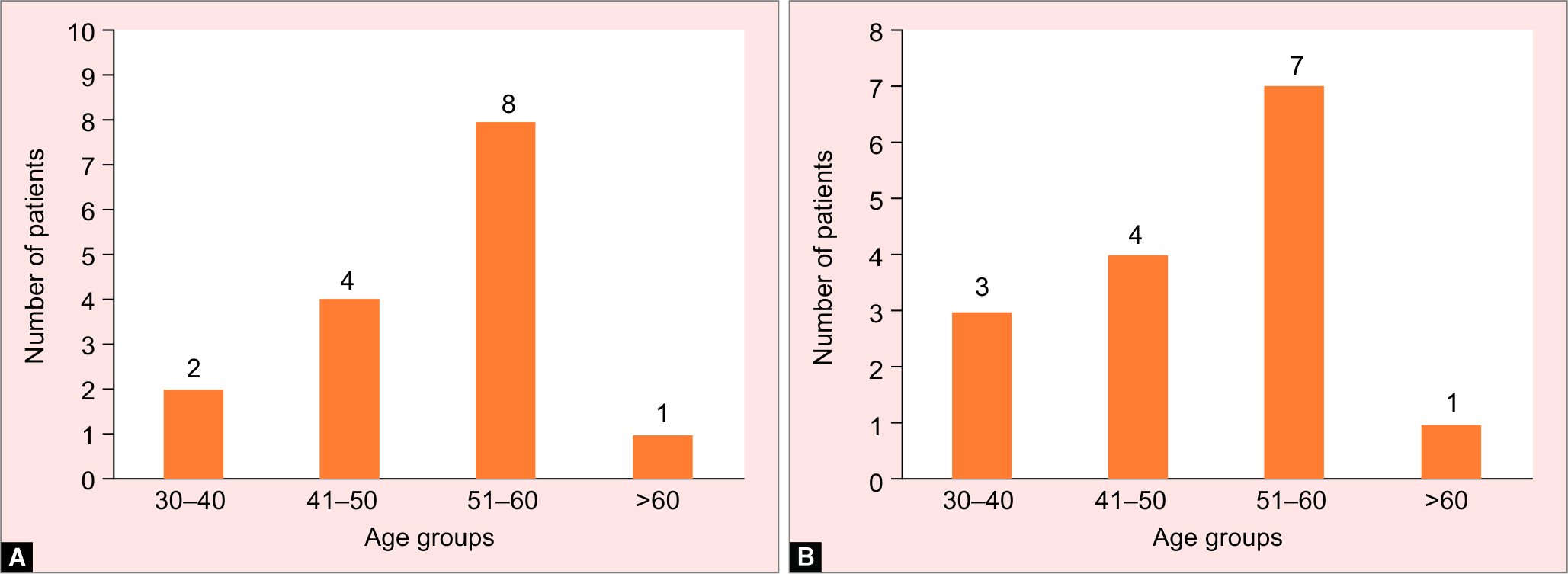
Figs 7A and B: (A) Age distribution in CTEP group; (B) Age distribution in patients of SILS TEP group
| Age-group | Number of patients |
|---|---|
| 30–40 | 3 |
| 41–50 | 4 |
| 51–60 | 7 |
| >60 | 1 |
SILS TEP Group
In our study of 30 patients, SILS TEP group consisted of 15 patients. There were three patients between the age-group of 30–40 years; four cases in the age-group of 41–50; seven cases between the age-group of 51–60; and one case above the age of 60 years. Majority of cases belong to age-group 51–60 years with mean age of 41.4 as is shown in the Table 1B and Figure 7B.
Sex Distribution
CTEP Group
In our study of 30 patients, CTEP group consisted of 15 patients. All the cases were males as is shown in the Table 2A and Figure 8A.

Figs 8A and B: (A) Sex distribution in patients of CTEP group; (B) Sex distribution in patients of SILS TEP group
| Sex | Number of patients |
|---|---|
| Males | 15 |
| Females | 0 |
| Sex | Number of patients |
|---|---|
| Males | 15 |
| Females | 0 |
SILS TEP Group
In our study of 30 patients, SILS TEP group consisted of 15 patients. All of cases were males; as is shown in the Table 2B and Figure 8B.
Site of Hernia
CTEP Group
In our study of 30 patients, CTEP group consisted of 15 patients. Right inguinal hernia was present in 10 cases. Left inguinal hernia was present in four cases. Bilateral inguinal hernia was present in one case. Most cases had right-sided inguinal hernia as shown in the Table 3A and Figure 9A.

Figs 9A and B: (A) Site of hernia in patients of CTEP; (B) Site of hernia in patients of SILS TEP
| Site of hernia | Number of patients | % age of patients |
|---|---|---|
| Right inguinal hernia | 10 | 66.66% |
| Left inguinal hernia | 4 | 26.66% |
| Bilateral inguinal hernia | 1 | 6.66% |
| Site of hernia | Number of patients | % age of patients |
|---|---|---|
| Right inguinal hernia | 8 | 53.33% |
| Left inguinal hernia | 5 | 33.33% |
| Bilateral inguinal hernia | 2 | 13.33% |
SILS TEP Group
In our study of 30 patients, SILS TEP group consisted of 15 patients. Right inguinal hernia was present in eight cases. Left inguinal hernia was present in five cases. Bilateral inguinal hernia was present in two cases. Most cases had right-sided inguinal hernia as shown in the Table 3B and Figure 9B.
Type of Hernia
CTEP Group
In our study of 30 patients, 15 cases underwent CTEP. Indirect inguinal hernia was seen in eight cases, while seven cases had direct inguinal hernia as is shown in Table 4A and Figure 10A.
| Type of hernia | Number of patients | % age of patients |
|---|---|---|
| Indirect inguinal hernia | 8 | 53.33% |
| Direct inguinal hernia | 7 | 46.66% |
| Type of hernia | Number of patients | % age of patients |
|---|---|---|
| Indirect inguinal hernia | 9 | 60% |
| Direct inguinal hernia | 6 | 40% |

Figs 10A and B: (A) Type of hernia in patients of CTEP; (B) Type of hernia in patients of SILS TEP
STEP Group
In our study of 30 patients, 15 cases underwent SILS TEP. Indirect inguinal hernia was seen in nine cases, while six cases had direct inguinal hernia as is shown in Table 4B and Figure 10B.
Operative Time
In our study of 30 patients, we calculated operating time from incision to wound closure and we found that the mean operative time of CTEP for unilateral hernia = 41.2 minutes and bilateral hernia = 64.6 minutes; whereas the mean operative time of SILS TEP for unilateral hernia = 42.8 minutes and bilateral hernia = 69.1 minutes with a p-value of 0.85 which is statistically insignificant as is shown in Table 5 and Figure 11.
| Type of hernia | CTEP time (mean) minutes | SILS TEP time (mean) minutes | p value |
|---|---|---|---|
| Unilateral | 41.2 | 42.8 | 0.85 |
| Bilateral | 64.6 | 69.1 |

Fig. 11: Chart showing the operative time of CTEP and SILS TEP for unilateral and bilateral hernias
Postoperative Complication
In our study of 30 patients, 15 patients underwent CTEP and 15 underwent SILS TEP. Seroma was seen in three cases of CTEP group and two cases of SILS TEP group. Hematoma was seen in one case of CTEP and none in SILS TEP group. Urinary retention was seen in one case of both CTEP and SILS TEP groups. However, there were no wound site infections in either group. The postoperative complications have been tabulated and compared as is shown in Table 6 and Figure 12.
| Postoperative complications | CTEP | SILS TEP | ||
|---|---|---|---|---|
| Number of patients | % age of patients | Number of patients | % age of patients | |
| Seroma | 3 | 20% | 2 | 13.33% |
| Hematoma | 1 | 6.66% | 0 | 0% |
| Urinary retention | 1 | 6.66% | 1 | 6.66% |
| Wound infection | 0 | 0% | 0 | 0% |

Fig. 12: Comparison of postoperative complications
Hospital Stay
In our study of 30 patients, 15 cases underwent CTEP and 15 cases underwent SILS TEP. The mean hospital stay of the patients undergoing CTEP was 19.2 hours and for SILS TEP group, it was 21.8 hours with a p-value of 0.97 which is statistically insignificant as is shown in Table 7 and Figure 13.
| Type of hernia | Mean hospital stay for CTEP in hours | Mean hospital stay for SILS TEP in hours | p value |
|---|---|---|---|
| Unilateral | 19.2 | 21.8 | 0.97 |

Fig. 13: Comparison of length of hospital stay
Time to Return to Normal (Nonsternous) Work
In this study of total 30 cases, we analyzed the time to return to work after CTEP and SILS TEP. It was observed that time to return to work was slightly lower in SILS TEP group than CTEP group. The time to return to work in CTEP 3.8 ± 0.8and SILS TEP 3.4 ± 1.2 as shown in Table 8 and Figure 14 with p-value of 0.3 which is statistically insignificant.
| Name of procedure | Time to return to work (in days) | Standard deviation |
|---|---|---|
| CTEP | 3.7 | 0.8 |
| SILS TEP | 3.3 | 1.2 |

Fig. 14: Comparison of time to return to normal (nonstrenuous) work after CTEP and SILS TEP procedure
Postoperative Pain Score
In our study of 30 cases, CTEP was performed on 15 cases and SILS TEP on 15 cases. The postoperative pain score was observed in each group at 6 and 24 hours using visual analogue scale (VAS) score. It was observed that the postoperative pain score was 3.1 and 2 for CTEP group at 6 and 24 hours, respectively. Similarly, the postoperative pain score was 2.8 and 1.2 for SILS TEP group at 6 and 24 hours, respectively, as is shown in Table 9 and Figure 15. The p-value was 0.5 at 6 hours and 0.32 at 24 hours.
| Visual analogue scale (VAS) | CTEP | SILS TEP |
|---|---|---|
| At 6 hours | 3.1 (±1.2) | 2.8 (±0.8) |
| At 24 hours | 2 (±1) | 1.2 (±1.1) |

Fig. 15: Comparison of postoperative pain score using VAS
Cosmesis
In our study of 30 cases, 15 cases underwent CTEP and 15 cases underwent SILS TEP. The cosmetic outcome was graded by the patient 1 month postoperatively on a scale of 1–5. It was observed that the mean of cosmetic results was 3.9 and 4.1 for CTEP and SILS TEP, respectively, as is shown in Table 10 and Figure 16 with a p-value of 0.23 which is statistically insignificant.
| Name of the procedure | Cosmetic results mean | Standard deviation |
|---|---|---|
| CTEP | 3.9 | ±0.8 |
| SILS TEP | 4.1 | ±0.9 |

Fig. 16: Comparison of cosmetic outcome in CTEP and SILS TEP procedures
Rate of Conversion to Open Technique
In our study of 30 patients of inguinal hernia undergoing CTEP/SILS TEP, there was no conversion to open technique.
Cost
In our study, the cost in SILS TEP group, using routine laparoscopic instruments was not statistically different from the CTEP group without compromising patient safety. However, the actual cost for SILS TEP when using specialized articulating instruments is significantly higher.
DISCUSSION
Inguinal hernia repair is one of the most common elective procedures performed in general surgery. The goal of hernia repair includes achieving effective repair, lowest possible recurrence, minimizing intraoperative and postoperative complications, rapid return to daily work, and reasons; various methods of inguinal hernia repair have been utilized over the past. The technique of herniorrhaphy has progressed from open to various laparoscopic techniques.
The present study was done to compare and analyze the results of laparoscopic CTEP and SILS TEP mesh repair for inguinal hernia. A total of thirty patients were included in the study. Fifteen patients were operated on by laparoscopic CTEP hernioplasty and other fifteen were operated on by laparoscopic SILS TEP hernioplasty.
Age
The most common age-group in both the methods was 51–60 years showing that groin hernia is most common in the middle age-group. In CTEP group, the mean age was 50.67 years. In SILS TEP group, the mean age was 41.40 years.
Wijerathne et al.8 in their study reported that the mean age of the patients undergoing CTEP was 50.3 and 47.2 years in patients undergoing SILS TEP.
Choi et al.9 observed in their study that the mean age in CTEP group was 57.5 years and for the SILS TEP group, it was 59.5 years.
Sex Distribution
All the patients in our study were males. CTEP group consisted of 15 patients, while the SILS TEP group also consisted of 15 patients.
Choi et al.9 reported that there were no female patients in either of their study groups.
Kim et al.10 reported in their study that most of the patients were males only accounting for 97% of cases. Two patients were female; statistically, there was no difference between the two groups as far as sex ratio is concerned. With these observations made, it is concluded inguinal hernias occur commonly in males.
Site of Hernia
In our study of 30 patients, most cases had a right-sided inguinal hernia. The CTEP group consisted of 15 patients. The right inguinal hernia was present in 10 (67%) cases. Left inguinal hernia was present in four (27%) cases. The bilateral inguinal hernia was present in one (7%) case. The SILS TEP group consisted of 15 patients. The right inguinal hernia was present in eight (53%) cases. Left inguinal hernia was present in five (33%) cases. The bilateral inguinal hernia was present in two (13%) cases.
Choi et al.9 observed in their study that most cases had a right-sided inguinal hernia (69%—CTEP group and 73%—SILS TEP group). However, 31 and 28% of cases of the CTEP group and SILS TEP group, respectively, had left-sided inguinal hernia.
Kim et al.10 in a study group of 60 patients with inguinal hernias observed that 51.66% of patients had right-sided hernias, 43.33% of patients had left-sided hernias, and 5% patients had bilateral hernias.
Our results were consistent with the literature to find right-sided inguinal hernia more common than left, then followed by bilateral hernia.
Type of Hernia
In our study of 30 patients, most cases had an indirect inguinal hernia. The indirect hernia was more common than the direct hernia, with a ratio of 08/15 (53%) in the CTEP group and 09/15 (60%) in the SILS TEP group.
Kim et al.10 in their study reported that indirect hernia was present in 40/63 (63%) of cases undergoing SILS TEP. The direct hernia was present in 23/63 (37%) of cases undergoing SILS TEP.
Tai et al.11 observed in their study that an indirect hernia was more common than a direct hernia, with a ratio of 69/152 (45.4%) in the CTEP group and 58/98 (59%) in the SILS TEP group. The direct hernia was present in 68/152 (44.7%) of cases undergoing CTEP and 39/98 (39%) of cases undergoing SILS TEP.
Thus, on analyzing the above study and present study, it is evident that our results are consistent with the above studies.
Operating Time
In our study, we observed that the mean operating time in the CTEP group was 41.2 and 64.6 minutes for unilateral and bilateral inguinal hernias, respectively. The mean operating time for SILS TEP was found to be 42.8 and 69.1 minutes for unilateral and bilateral inguinal hernias, respectively. It was, however, observed that there was no statistically significant difference in operating time (p-value = 0.85).
Tai et al.11 in their study concluded that the mean operative time in the CTEP group was 58.6 and 62.5 minutes for unilateral and bilateral inguinal hernias, respectively; while the mean operative time for SILS TEP was 82.3 and 68.3 minutes, respectively.
Wijerathne et al.12 concluded in their study that the mean operative time for unilateral inguinal hernias in CTEP and SILS TEP techniques was 50.5 and 63.5 minutes, respectively.
Choi et al.,9 in their study concluded that the mean operative time for CTEP was 41.6 minutes for unilateral hernias; while for SILS TEP, the mean operative time was 61.7 minutes.
Postoperative Complications
Overall complications were slightly more in the CTEP method than in SILS TEP method five (33.3%) vs three (20%). The most common complication was postoperative seroma in both groups. Three (20%) patients in the CTEP group and two (13%) patients in the SILS TEP group developed postoperative seroma which was noticed at discharge and also at 1-week follow-up, which was conservatively managed. One (7%) patient in the CTEP group developed hematoma (managed conservatively). One (7%) patient in both groups had postoperative urinary retention, managed by catheterization. Observations made in our study were consistent with studies by Choi et al.,9 in their study have reported overall 24% of complications in the CTEP group and 16% in the SILS TEP group. Postoperative seroma developed in 20% of cases in both groups. Urinary retention developed in 6 and 2% cases in CTEP and SILS TEP, respectively.
Wijerathne et al.8 reported that postoperative seroma was the most common complication in both methods. All patients with seroma were managed conservatively without any intervention. Postoperative seroma developed in 17% of cases undergoing CTEP and 8% of cases undergoing SILS TEP.
Thus our results are consistent with the above-given studies.
Hospital Stay
Orals were started as soon as postoperative nausea was over and the patient felt hungry. Patients in both groups were advised early ambulation. As the patients became ambulant, tolerated orals, and voided urine, they were discharged. The mean postoperative hospital stay in CTEP repair was 19.2 hours and in SILS TEP repair 21.8 hours; (p-value of 0.97—statistically insignificant).
Wijerathne et al.8 reported the mean hospital stay of 19.7 hours in CTEP group and in SILS TEP group, it was 20.5 hours.
Lomanto et al. reported in their study that the mean hospital stay for CTEP was 19.7 hours and for SILS TEP, it was 22.1 hours.
Time Until Return to Normal Daily Work
In our study, the average time to resume normal nonstrenuous work was 3.7 ± 0.8 days in CTEP repair and 3.3 ± 1.2 days in SILS TEP repair. Thus CTEP group had the almost same time to resume normal work as the SILS TEP group.
Tai et al.11 observed that patients operated by CTEP repair and SILS TEP repair return to normal work after a mean of 3.8 and 3.4 days which was statistically nonsignificant.
Thus our observations were consistent with the results of other studies.
Postoperative Pain
The postoperative pain was calculated using a VAS score. VAS score was almost the same in CTEP and SILS TEP procedures. VAS score was calculated at 6 and 24 hours after surgery. The mean VAS score at 6 hours in the CTEP group was 3.1 ± 2.8 and in the SILS TEP group 2.8 ± 0.8. VAS score at 24 hours was 2 ± 1 and 1.2 ± 1.1 for CTEP group and SILS TEP group, respectively. At 6 hours, p-value = 0.5 and 0.32 at 24 hours after surgery.
Wijerathne et al.8 concluded that pain score (VAS) at 6 hours, 24 hours, 1 week, 4 weeks, 3 months, and 6 months after surgery was slightly higher in the CTEP group compared to SILS TEP group. VAS score at 6 hours in CTEP was 2.6 ± 1.3 and in the SILS TEP group 2.1 ± 1.5. VAS score at 24 hours was 2.1 ± 1.5 in the CTEP group and SILS TEP group 1.5 ± 1.5. At 6 hours, p-value = 0.146 and 0.067 at 24 hours after surgery; hence the difference between CTEP and SILS TEP was not statistically significant.
The observation made in our study favored SILS TEP to be less painful than CTEP, however, statistically insignificant. The findings were consistent with the observation made by Wijerathne et al. when VAS is compared at 6 and 24 hours.
Cosmesis
The cosmetic outcome of the patients was compared after 1 month of surgery. Cosmetic results were graded subjectively 1 month postoperatively using the following range of choices: 5 (very satisfied), 4 (satisfied), 3 (acceptable), 2 (dissatisfied), and 1 (very dissatisfied) (Fig. 17). The mean cosmetic result was 3.9 ± 0.8 in the CTEP group and 4.1 ± 0.9 in the SILS TEP group. The p-value = 0.14 which is statistically insignificant.

Figs 17A and B: Postoperative scar at (A) 1 week; (B) 2 months
Tai et al.11 observe that the cosmetic outcome graded objectively by the patient was 3.9 ± 0.7 and 4.1 ± 0.8 in CTEP and SILS TEP groups, respectively. The p-value = 0.14 which is statistically insignificant.
Thus concerning cosmetic outcomes, our results are consistent with the above study.
Conversion to Open
In our study of 30 patients with inguinal hernia undergoing CTEP/SILS TEP, there was no conversion to open technique.
Choi et al.9 in his study “Single-port versus conventional three-port laparoscopic totally extraperitoneal inguinal hernia repair: a randomized controlled trial” had no conversion to the open technique.
Cost
In our study, the cost in the SILS TEP group, using routine laparoscopic instruments was not statistically different from the CTEP group without compromising patient safety. However, the actual cost for SILS TEP when using specialized articulating instruments is significantly higher.
Observation made in our study was consistent with the study by Rajapandian et al.,13 who in their study “single incision versus conventional laparoscopic inguinal hernia repair: A matched comparison” concluded that the cost of SILS TEP using conventional laparoscopic instruments in a resource-poor and cost-sensitive country like India was not statistically different from the conventional group without compromising the safety of the patient.
CONCLUSION
The outcome of inguinal hernias using laparoscopic modality is associated with good results in both techniques. SILS TEP inguinal hernia repair using conventional laparoscopic instruments is a safe and feasible alternative to CTEP in experienced hands. The outcomes of SILS TEP for operation time, postoperative complication, duration of stay, time until return to normal nonstrenuous activity, and conversion to open are comparable to CTEP.
However, the approach provided advantage in terms of cosmesis and postoperative pain using VAS score.
ORCID
Yaser Hussain Wani https://orcid.org/0000-0001-5249-2164
Safoora Wani https://orcid.org/0000-0002-3186-4413
REFERENCES
1. Liu N, Greenberg JA, Brooks DC. Chapter 11: inguinal hernia. In: Maingot’s abdominal operations. 13th ed. McGraw Hill Education; 2019. p. 193.
2. Malangoni MA, Rosen MJ. Hernias. In: Sabiston textbook of surgery: the biological basis of modern surgical. 20th ed. Elsevier; 2008. p. 1092–1093.
3. Kingsnorth A, LeBlanc K. Hernias: inguinal and incisional. Lancet 2003;362(9395):1561–1571. DOI: 10.1016/S0140-6736(03)14746-0.
4. Hernias G. Surgical-tutor.org website. Available from: (a href="http://www.surgical-tutor.org.uk/specialities/general/hernias.htm")http://www.surgical-tutor.org.uk/specialities/general/hernias.htm(/a) [Accessed May 13, 2008].
5. Wantz GE. Abdominal wall hernias. In: Schwartz SI, editor. Principles of Surgery. 7th ed. New York, NY: McGraw-Hill; 1999. p. 1585–1611.
6. Read RC. The contributions of Usher and others to the elimination of tension from groin herniorrhaphy. Hernia 2005;9(3):208–211. DOI: 10.1007/s10029-005-0322-1.
7. Neumayer L, McGregor DB, Mann B. Abdominal wall, including hernia. In: Lawrence PF, editor. Essentials of general surgery. 4th ed. Baltimore, MD: Lippincott, Williams & Wilkins; 2006. p. 225–237.
8. Wijerathne S, Agarwal N, Ramzi A, et al. Single-port versus conventional laparoscopic total extra-peritoneal inguinal hernia repair: a prospective, randomized, controlled clinical trial. Surg Endosc 2016;30(4):1356–1363. DOI: 10.1007/s00464-015-4378-4.
9. Choi BJ, Jeong WJ, Lee IK, et al. Single-port versus conventional three-port laparoscopic totally extra peritoneal inguinal hernia repair: a randomized controlled trial. Hernia 2016;20(6):789–795. DOI: 10.1007/s10029-016-1499-1.
10. Kim JH, Park SM, Kim JJ, et al. Initial experience of single port laparoscopic totally extraperitoneal hernia repair: nearly-scarless inguinal hernia repair. J Korean Surg Soc 2011;81(5):339–343. DOI: 10.4174/jkss.2011.81.5.339.
11. Tai HC, Lin CD, Chung SD, et al. A comparative study of standard versus laparoendoscopic single-site surgery (LESS) totally extraperitoneal (TEP) inguinal hernia repair. Surg Endosc 2011;25(9):2879–2883. DOI: 10.1007/s00464-011-1636-y.
12. Wijerathne S, Agarwal N, Ramzy A, et al. A prospective randomized controlled trial to compare single-port endo-laparoscopic surgery versus conventional TEP inguinal hernia repair. Surg Endosc 2014;28(11):3053–3058. DOI: 10.1007/s00464-014-3578-7.
13. Rajapandian S, Bushan C, Sabnis SC, et al. Single incision multiport versus conventional laparoscopic inguinal hernia repair: a matched comparison. J Minim Acess Surg 2018;14(1):44–51. DOI: 10.4103/jmas.JMAS_30_17:10.4103/jmas_30_17.
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.