|
CASE REPORT |
https://doi.org/10.5005/jp-journals-10033-1514
|
Melena Post-laparoscopic Appendicectomy—One of a Kind: A Rare Case Report
1,2Department of General Surgery, Mahatma Gandhi Medical College and Research Institute, Puducherry, India
Corresponding Author: Siddartha Gowthaman Subramaniyan, Department of General Surgery, Mahatma Gandhi Medical College and Research Institute, Puducherry, India, Phone: +91 9894098987, e-mail: sidhugowtham@gmail.com
How to cite this article: Subramaniyan SG, Akshaya HB. Malena Post-laparoscopic Appendicectomy—One of a Kind: A Rare Case Report. World J Lap Surg 2022;15(3):260–261.
Source of support: Nil
Conflict of interest: None
Received on: 25 October 2021; Accepted on: 06 September 2022; Published on: 07 December 2022
ABSTRACT
Melena usually occurs as a result of an upper gastrointestinal bleed, rarely it can be due to bleeding in the small intestine and ascending colon. Appendicectomy is one of the safest procedures done with overall minimal complication rate of about 5%. In this article, we have discussed about melena post-laparoscopic appendicectomy, which is one of the rarest complications of the procedure.
Keywords: Appendicectomy, Laparoscopy, Melena.
INTRODUCTION
Appendicectomy can be done by open or laparoscopical approach, and is the commonest surgery performed with a very minimal complication rate.1
The postoperative complications are quite rare, with a mean rate of 4.6 and 3.3%, respectively, which are intra-abdominal abscesses, stump leakage, stump appendicitis, surgical site infections, seromas, wound rupture, intestinal damage, medical complications, small-bowel obstruction due to the formation of adhesions, and paralytic ileus.2
Though cases with rectal bleeding post appendicectomy had been reported in the literature, melena post appendicectomy is one kind of complication as melena as a cause of lower intestinal bleed is itself a rare complication.3
In this article, we had discussed about melena that occurred post laparoscopic appendicectomy in a young male patient and its management.
CASE DESCRIPTION
A 28-year-old male with no known comorbidities or past surgical history, came to the surgical outpatient department with complaints of right lower abdominal pain, pricking type of pain, intermittent, and no aggravating or relieving factors. He also complained of 2 episodes of vomiting containing food particles, non-bilious, and non-blood-tinged. History of fever, 1 episode, low grade, not associated with chills or rigors, resolved spontaneously. On examination, the abdomen was soft, tenderness present over the right iliac fossa, with rebound tenderness, bowel sounds heard, and hernial orifices free. No significant findings in per-rectal examination following which ultrasound abdomen was suggestive of acute appendicitis. After routine investigations, the patient was taken up for laparoscopic appendicectomy under general anesthesia. Intraoperative inflamed appendix was found in the right iliac fossa. Histopathology of the specimen shows an appendix with mucosal ulceration. Lamina propria shows dense inflammatory composed predominantly of lymphocytes and eosinophils extending up to the muscularis propria. Serosa shows congested blood vessels (Fig. 1).

Figs 1A and B: Histopathology of specimen: Lamina propria shows dense inflammatory composed predominantly of lymphocytes and eosinophils extending up to the muscularis propria. Serosa shows congested blood vessels
The patient on postoperative second day complained of pain, black-colored stools suggestive of melena following which UGI scope showed normal study and CECT abdomen was taken, which showed postoperative inflammatory changes in the form of mild bowel-wall enhancement, mesenteric fat stranding, and minimal interbowel-free fluid at the ileocecal junction in the right iliac fossa. No obvious arterial bleed or pseudoaneurysms were noted. Mild post-op arterial phase blush near the post-op region was seen which might be suggestive of source of melena (Fig. 2).
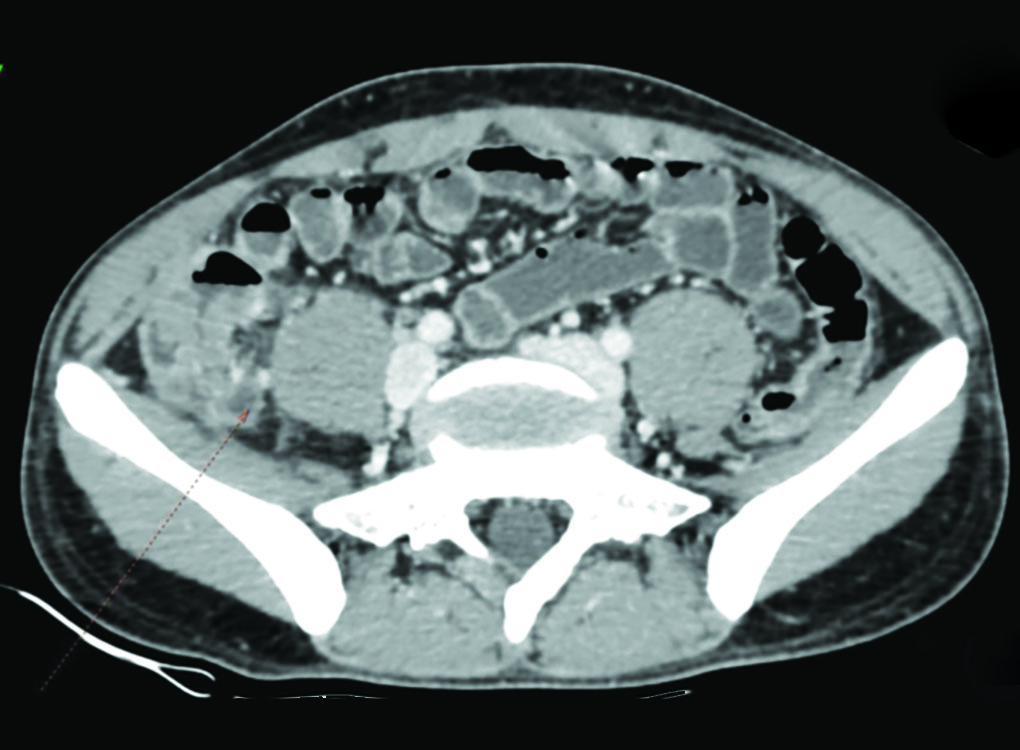
Fig. 2: CECT abdomen was taken which showed postoperative inflammatory changes in the form of mild bowel wall enhancement, mesenteric fat stranding, and minimal interbowel-free fluid at the ileocecal junction in the right iliac fossa. No obvious arterial bleed or pseudoaneurysms were noted. Mild post-op arterial phase blush near the post-op region was seen, which might be suggestive of the source of melena
Melena post appendicectomy is one of the rarest complications. Only a handful number of cases have been reported about lower GI bleed post appendicectomy as mentioned by Koimtzis et al.,4 but melena post appendicectomy had never been reported in literature. In our case, upper gastrointestinal bleeding was ruled out as the cause of melena by upper GI endoscope. CECT abdomen ruled out any active bleed in the abdomen or peritoneal collection, which would have caused melena. As other causes are ruled out, the probable cause of melena in our case would be stump bleed where the patient was closely monitored, where the symptoms resolved spontaneously after 5 days. Colonoscopy can also be considered if the patient develops the complication at a later stage.
CONCLUSION
In summary, we have presented a very unusual case of melena post appendicectomy. Although this type of complication is rarest, but if it is left unattended, the patient might end up with serious complications, also, unnecessary intervention may result in serious morbidity for the patient.
REFERENCES
1. Kirby A, Hobson RP, Burke D, et al. Appendicectomy for suspected uncomplicated appendicitis is associated with fewer complications than conservative antibiotic management: a meta-analysis of post-intervention complications. J Infect 2015;70(2):105–110. DOI: 10.1016/j.jinf.2014.08.009.
2. Andersson RE. Short-term complications and long-term morbidity of laparoscopic and open appendicectomy in a national cohort. Br J Surg 2014;101(9):1135–1142. DOI: 10.1002/bjs.9552.
3. Vo N, Hall FM. Severe post appendectomy bleeding. Am Surg 1983;49(10):560–562. PMID: 6331778.
4. Koimtzis G, Sapalidis K, Koletsa T, et al. Massive endoluminal bleeding from the invaginated appendiceal stump after appendectomy: a unique case of gastrointestinal bleeding. ProClinS Surgery and Procedures 2018;1(1):1–5.
________________________
© The Author(s). 2022 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.